Breast implant revision – changing implants to on TOP of the muscle

In my practice, I see many women who not entirely happy with their results after having breast implant surgery elsewhere. Their surgery may be reconstructive, for instance after mastectomy or lumpectomy for breast cancer, or a cosmetic breast augmentation.
Why are implants placed under the muscle?
Many Plastic Surgeons place breast implants under the pectoralis major muscle (known as the “Pec” muscle) because they believe it to be a better option. While there are some rare instances where I agree (mostly reconstructive where the incision is right in the middle of the breast), I usually AVOID placing implants under the muscle because of the results I see in women seeking breast revision. Learn more about why I prefer the subglandular position for most breast augmentation patients here.
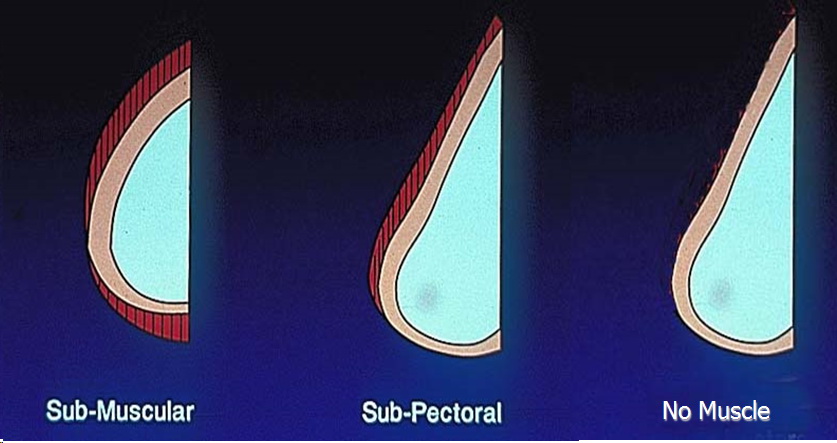
If breast implants are placed completely under the muscle, they result in a tight half-dome shape not desired by most women! Implants can be placed partially under the muscle, but contraction of the pectoralis will cause an upward and outward deformity during muscle animation. If the implant is placed completely ON TOP of the muscle, animation deformity and muscle tightness is avoided.
What do patients complain of when their implants are under the pectoralis muscle?
These patients often complain about their implants feeling tight, sitting too high or too wide, and in particular about a change in shape whenever they use their arms. See the images below for examples of the “motion or flexion deformity”, a deformation of the breast skin when the pectoralis major muscles are contracted.
Some women complain of chronic pain or discomfort related to their implants being under their muscles. Incredibly, these women are told by their surgeons to “just stop doing upper body exercises and going to the gym”. REALLY? Yikes!
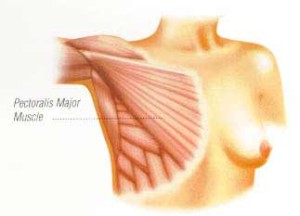
The pectoralis major muscle is a flat chest muscle that serves the function of moving the arm toward the body, and is not really designed to be stretched out over a breast implant!
The pectoralis major muscles are the largest chest muscle and they are involved in ALL upper body motions. Their function is for moving the arm and shoulder, and they have a straight vector of pull, in an up-and-out direction, as illustrated above by the direction of the muscle fibers. Because of this anatomy, sub-muscular implants tend to migrate too high and too far apart over time due to repeated muscle contraction over time.
It is impossible to NOT use the pectoralis muscles during activities of daily living (unless you are paralyzed from the neck down or are a department store mannequin!). Advising patients to stop using their muscles or to cease exercise is completely unacceptable in my opinion. I cannot imagine counseling patients that there is no other way…

At rest, implant reconstruction under the muscle can look somewhat normal.

However, with flexion of the pectoralis muscles, the skin contracts over the implant and deformity results. Most women are self-conscious about the motion deformity.
So what can be done? Can the situation be corrected? Simply, YES!
Regardless of whether the implants were put under the muscle during a reconstructive procedure or for a cosmetic breast augmentation, it is possible to have a revision of the augmentation or reconstruction to achieve more aesthetic, natural, symmetric and comfortable results.
In this outpatient surgery that usually takes two to three hours and requires drains for around a week postop, the pectoralis muscle is returned to the chest wall and the implant is moved on top of the muscle.
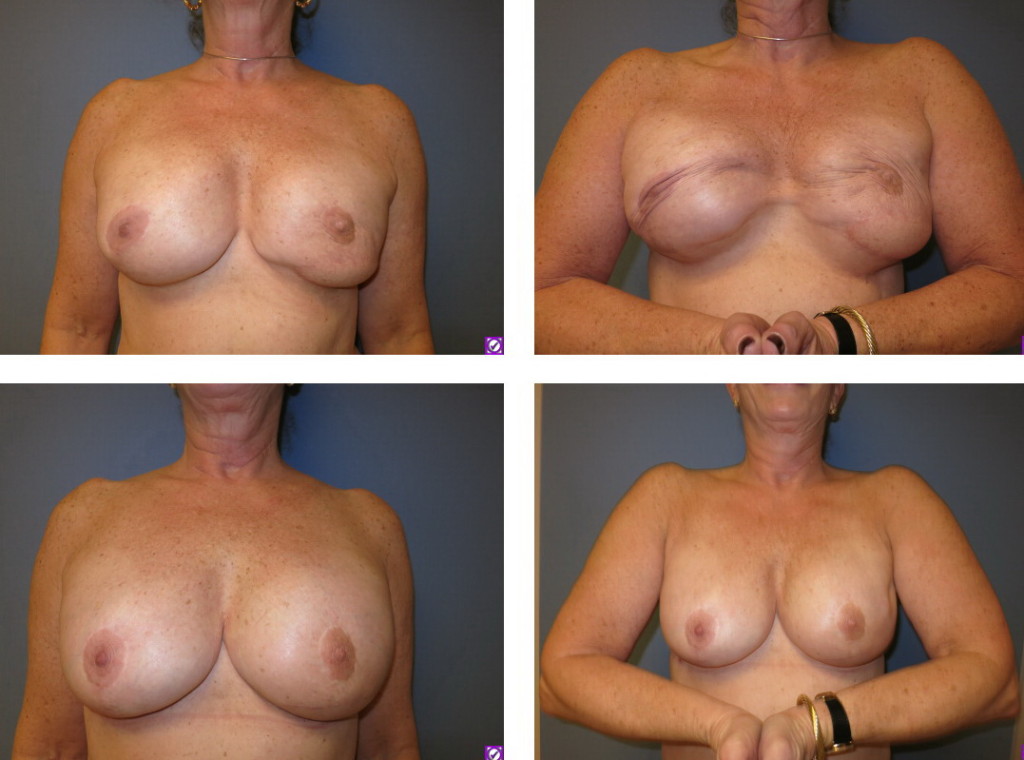
Before and after surgery that replaced the pectoralis major chest muscle to the chest wall after mastectomy and implant reconstruction. On the left is the muscles are at rest; on the right, flexion of the muscles. The deformity and associated muscle tightness and discomfort both during animation and at rest were alleviated with surgery.
The muscle is sutured back to its normal anatomic position on the chest wall using thick, braided, slowly dissolving sutures from the muscle to the tissue underneath. Patients often ask whether the muscle is all stretched out and whether it will need to trimmed or anything else special be done to get it back into place. The muscle happily returns immediately to its flat, relaxed state on the chest wall, which is where it really wants to be!
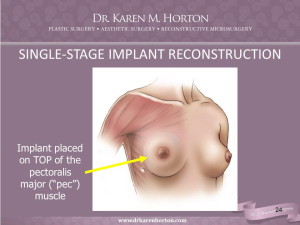
Breast implants can be placed directly on top of the muscle for a more natural result that does not result in muscle contraction deformity or discomfort. After a mastectomy, the implant will be in a subcutaneous position. The incision is underneath the breast for nipple-sparing mastectomies.
Putting the pectoralis muscle back under the implant corrects the motion/flexion deformity and usually cures the sensation of pulling, tightness or discomfort if it is related to muscle strain or contraction.

Cosmetic breast augmentation where the implant was placed under the muscle. The pectoralis pulls the implant upward, and the breast tissue droops off the implant, creating the “Snoopy nose” deformity, also called the “waterfall deformity” by some surgeons.

The pectoralis muscle was returned to the chest wall and the same implant was placed on top of the muscle. This provided a natural breast shape and corrected the visible deformity and associated muscle strain and physical discomfort.

Oblique view of a breast augmentation patient with implants under the muscle. She was self-conscious about the high placement of her implants and was told to stop exercising by her surgeon.

3 weeks after returning the chest muscle to its location on the chest wall and putting the breast implant on top. A normal breast contour results and she has returned to full exercise and weight lifting!
What is the recovery after moving breast implants from under to on top of the muscle?
Patients can usually return home the day of surgery, which takes 2-3 hours on average under general anesthesia. If reconstruction patients are traveling far from out of town, I usually keep them in the hospital overnight and discharge them the next day to save them from paying for a hotel that night.
Since the muscles have been restitched to their location on the chest wall, it is important to keep pec muscle activity relatively quiet for at least 4 weeks after surgery. This means no lifting more than 5 pounds for at least a month, no aggressive physical exercise for 4-6 weeks, and usually 2 weeks off work. Learn more about recovery after breast surgery here.
Recovery is surprisingly NOT very painful, as reported by most of my patients. Often, the reason they seek revision surgery is because of chronic discomfort or tightness, and this is usually gone as soon as they wake up! The pectoralis muscles are very vascular and have a robust blood supply and sensory nerves supplying them – thus, cutting them off the chest wall and chronically stretching them out over an implant intuitively creates tension in the chest and related discomfort.
Most women remember the amount of pain and discomfort associated with their initial surgery to place the implants under the muscle. Thankfully, when we remove the implant from under the muscle and place it on top, this relieves the tension and the muscle is happy to be back in its normal position!
Recovery after returning the muscles to their normal anatomic state usually hurts much less than the original under-the-muscle surgery. Even though we are handling the muscle to replace it to the chest wall, dissection of the muscle is very gentle, and it is performed under loupe magnification (Microsurgical technique). The level of postoperative discomfort is usually described as a “1-3 / 10 pain” as opposed to the “8-10 / 10 pain” they experienced during their tissue expansion or sub-muscular breast augmentation.

Before surgery, the right pectoralis muscle creates severe deformity when it is flexed. The left breast drooping from age and gravity.

The right pectoralis muscle has been returned to the chest wall and the implant is now placed on top of the muscle. The left breast has been lifted for better symmetry.
Can the muscles be returned to the chest wall even years after the initial surgery?
Yes! There is NO time limit to when a breast revision surgery can be performed. If the surgery was done for breast reconstruction after cancer treatment or for prophylactic reasons (BRCA gene positive women or a strong family history of breast cancer), a breast revision will be covered by insurance. For cosmetic revisions, it is not covered by insurance and patients are responsible for paying for surgery themselves.
Do the breast implants need to be switched out or exchanged during breast revision and placement on top of the muscle?
It is not necessary to change the implants to another size or style during breast revision, unless a different look or result from the implant is desired. For instance, if a fuller or smaller result is desired, the implant might be changed, or a saline implant could be switched to silicone gel to have less rippling or wrinkling of the implant in reconstructive cases.
Are there any disadvantages of placing breast implants on top of the muscle?
The only potential disadvantage is the appearance of RIPPLING of the implant, which results from seeing folds of the implant through very thin skin – usually after a mastectomy where the breast surgeon removed much of the subcutaneous fat in the upper pole of the breast. Rippling means the implant is soft and the skin is very thin over top. Rippling usually only occurs in reconstructive patients – it is rare in cosmetic breast augmentations, even if the patient is very thin.
Can anything be done to conceal rippling of an implant in reconstructive situations?
Read my web page about the controversial topic of free fat grafting to the breasts and a a recent blog post that discusses the use of fat grafting in cosmetic situations to hear my thoughts on this topic.
See my before-and-after breast augmentation gallery for images of implants on top of the muscle (known as the subglandular position) in many thin, athletic patients who do not want to look fake but seek a natural result. Even if there is little breast tissue, the implants are placed in a manner that the skin drapes naturally over the implant to create a teardrop shape and proportional aesthetic result.
Likewise, the revision breast surgery before-and-after gallery shows many other examples of implants that have been converted from under the muscle to on top of the muscle, with a dramatically more aesthetically appealing result in most cases – and relief of the discomfort or deformity that brought these patients to my office in the first place.
Implants under the muscle usually do NOT ripple because the muscle is tight over top of the implant! Trading muscle tightness and tension for potential rippling is a potential trade-off that I discuss with detail with my patients when they are considering a breast revision with conversion of their implants to on top of the muscle.

This patient was told by her surgeon “you look fine in clothes”. This was unacceptable to the patient, and to me! The pectoralis muscle pulls the implant upward and outward, following its vector of action.

Both pectoralis muscles were returned to the chest wall and and implants were placed on top of the muscle. Nipple and areolas were reconstructed using the local flap technique and medical tattoo for better symmetry. Results are not perfect, but much better! And physical discomfort was immediately relieved.

It’s no wonder that implants under the muscle migrate to this position – see the anatomy diagram that shows where the muscle lies on the chest wall and its muscle fiber orientation.

Oblique view following replacement of chest muscles to their normal position and placement of implants on top of the muscle.
Here is a quote from a patient who is a carrier for the BRCA gene. She sought a bilateral prophylactic mastectomy to decrease her lifetime risk of breast cancer. The local surgeons only offered her an under-the-muscle multiple-stage tissue expander and implant reconstruction, which resulted in a severe muscle contraction deformity and physical disability. Here are her thoughts:
“I was highly athletic prior to my mastectomy with standard sub-pectoral reconstruction. I was in a constant state of pain from the day I got my mastectomy until the afternoon I woke from my revision a year later. I chose to seek out this revision procedure as I was no longer able to perform daily tasks without pain associated with the use of my chest muscles.
In the year leading up to my revision I sought out the professional opinion of not only my original reconstructive surgeon, but three other surgeons before finding Dr. Horton. All but one of the other surgeons told me that I needed to get used to it and that it was my new normal. This was not a valid answer for me.
Since having my revision, and being cleared by Dr. Horton to resume normal use, I am back to daily living, working out daily and I don’t even give my chest a second thought, unless I am doing push ups, planks and burpees, I am still getting the hang of those.”
 There are no right or wrong answers in breast reconstruction or breast augmentation techniques. Most women who are interested in revision of their breast implants are doing so because of physical discomfort or deformity with muscle motion.
There are no right or wrong answers in breast reconstruction or breast augmentation techniques. Most women who are interested in revision of their breast implants are doing so because of physical discomfort or deformity with muscle motion.
For women who do not have any of these symptoms, then they are just fine and don’t need ANY surgery! I would never recommend surgery if it was not indicated for pain, deformity or patient dissatisfaction.
To learn more about revision breast surgery and placement of implants on top of the muscle, visit me in person by completing our online consultation request form or call 415-923-3067 to schedule a consultation at your convenience.
My aim is “to educate, inform and empower” all patients to learn about their options so that they can make the very best decision for what is right for their bodies and their lifestyle!